THE FROGGYMOUTH CONCEPT IN A FEW WORDS
THE PASSIVE APPROACH
IS A FUNCTIONAL REHABILITATION METHOD
WHICH DOES NOT REQUIRE ANY ACTIVE PARTICIPATION FROM THE PATIENT.
It was theorized as anoetic functional rehabilitation*, by Doctor PATRICK FELLUS, ODF specialist,
at the Robert Debré Hospital in Paris in 2011.
Its therapeutic goal is to automate new praxis by inhibiting dysfunctional circuits, and to establish a protocol based on current neuroscientific data.
The reference work on the subject was published in 2020 by Doctor FELLUS:
YOU CAN ALSO FIND THE CONCEPT IN REPLAY:
Conference by Dr. Fellus
for dental specialists (2h23)
Introduction for speech therapists and paramedical professionals by Samantha Weaver.
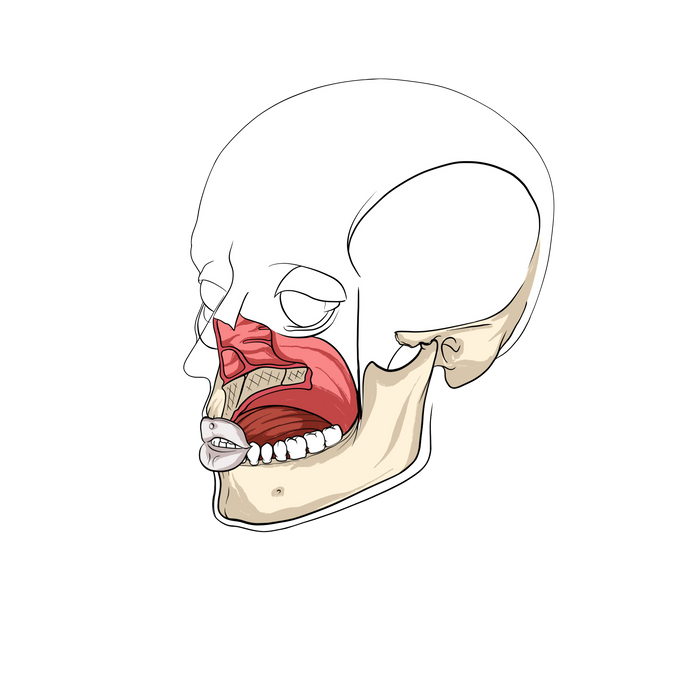
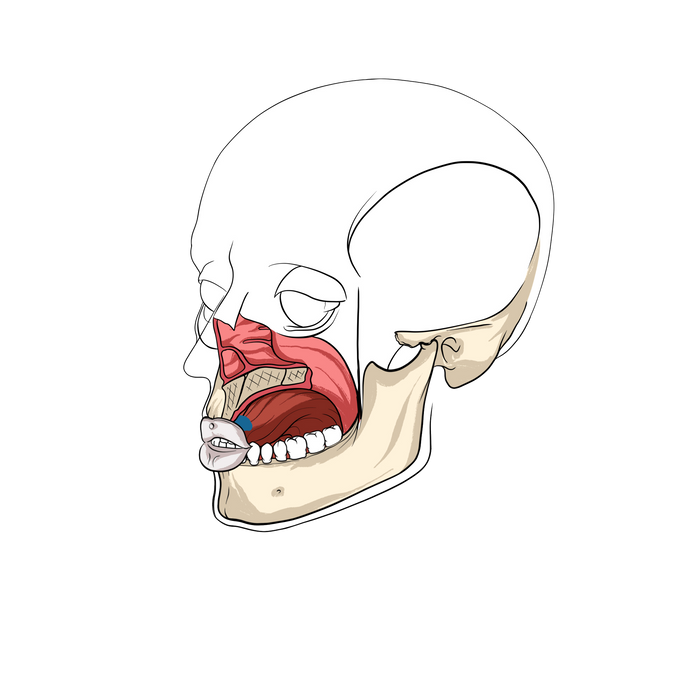
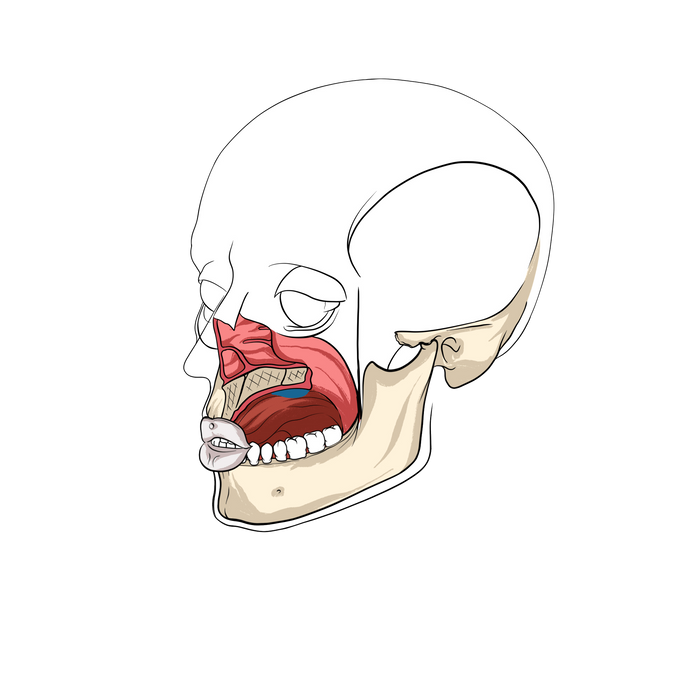
ATYPICAL DEGLUTITION, OR PRIMARY DEGLUTITION, TAKES PLACE IN TWO STAGES.
1. SUCKING REQUIRES A LIP SEAL IN ORDER TO CREATE NEGATIVE PRESSURE INSIDE THE ORAL CAVITY. THE LIP AND CHIN MUSCLES CONTRACT.
2. A LINGUAL BACK AND FORTH TO SWALLOW BY PRESSURE DIFFERENCE.
BUT…




HOW DO WE MOVE FROM INHIBITION OF ATYPICAL SWALLOWING TO CORRECTING THE POSITION OF THE TONGUE AT REST?